

Clinical Anatomy
Author(s):
Updated:
FEB 08, 2021
Languages:
Read
INTRODUCTION
The donkey has adapted to the need to feed on abrasive foods and has a series of anatomical differences to horses and ponies that are related to this adaptation. It is important to be aware of these differences, both for diagnosis and for treatment.
This chapter will cover the following subjects:
Key points
-
The cheek teeth are highly evolved to be a very efficient start to the digestive process, grinding rough, fibrous ingesta into particles for swallowing.
-
Eruption times for donkeys teeth are commonly 6 – 8 months later than the horse and pony, but there is considerable variation across the breeds.
-
Professionals need to be aware of the species specific anatomy.
-
The average faecal fibre length is a good indicator of dental disease.
Donkeys, horses and ponies have evolved in a similar way over millions of years, allowing them to survive as prey, but also allowing their adaptation from a diet of soft, leafy plant material, to more coarse vegetation. Their digestive system is primarily designed to obtain energy from a forage diet of grasses and other plant material, consumed steadily throughout the day. This has influenced the anatomy of the oral cavity.
The donkey has evolved to live in semi-arid environments with only poor quality, sparse vegetation.
ANATOMY OF THE ORAL CAVITY
Modern equids have a series of anatomical features in the head and oral cavity directly related to the need to feed on abrasive foodstuffs. The following list describes some of those anatomical features seen in the donkey, allowing a better understanding of the functional performance and also the complexity of the donkey’s head.
Donkeys have:
-
smaller brain cases and olfactory lobes
-
a longer preorbital region than postorbital region. This is a result of the elongation of the head, leading to a long oral cavity but also a complex sinus system. These structures are anatomically close and disorders affecting the oral cavity may also affect the sinuses
-
long-crowned molarised cheek teeth (CT) (hypsodont teeth), working as a functional unit of 6 CT per row (3 premolars and 3 molars, and excluding the wolf teeth)
-
diametrically opposed reserve crown at the rostral (pointing caudal) and the caudal (pointing rostral) CT, as well as the curvature of the last molars (11s), maintaining tight apposition of all CT at the clinical crown and occlusal surface
-
the curve of Spee (curvature of the mandibular occlusal plane) is quite noticeable in some donkey breeds, so an accentuated curve of Spee should be treated as a variation of normal conformation.
-
Differentiate the normal curve of Spee from overgrowths of the mandibular 11’s by palpating and visualising the distance from the mesial and distal aspects of the occlusal surface to the gingiva and ramus
-
Uniform clinical crown height in balance with the rest of the mandibular CT in addition to the maxillary counterparts would be assumed to be normal, whereas an imbalance of crown height at the mesial and distal aspects or disproportionate lack of crown height of the maxillary counterpart indicates dental overgrowth
-
-
a more acute incisor arcade than horses; with tight rostro-mesial compression from the 03s, which allows the incisor arcade to act as a single unit and may contribute to the commonly observed ventral curvature
-
hypsodont teeth with a continuous eruption rate of approximately 3–4 mm/year on average, followed by a similar wear rate (in correct feeding conditions), ensuring the presence of a clinical crown with a constant size inside the oral cavity
-
a continuous remodelling process of the nasal sinus as a direct consequence of the continuous eruption process of the CT, mainly those in direct contact with CT – rostral and caudal maxillary sinus
-
a greater degree of anisognathia – i.e. the maxilla is approximately 30% wider than the mandible (5–7% wider than in horses) at its widest point, although the disproportion of width appears to stem from a narrower straight mandible rather than a wider maxilla. This higher degree of anisognathia may be related with a need to have a wider lateral excursion movement, due to the need to chew very rough forage. This anatomical feature may contribute to the presence of enamel overgrowths as physiological or pathological structures in donkeys
-
significant differences in morphology between maxillary and mandibular CT; maxillary CT present greater surface area and contain more enamel in the form of mesial and distal infundibula
-
possible communication between the rostral and caudal maxillary sinuses as they are incompletely divided by a ventrally located low bony ridge which does not extend dorsally enough to divide both sinuses.

Lateral view of a young adult donkey skull.

Intraoral view of normal, healthy teeth in a donkey.
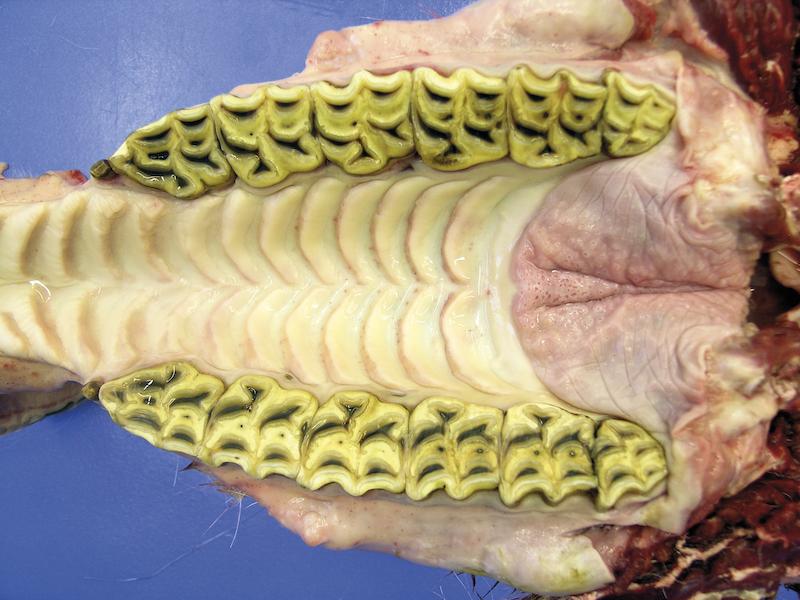

Occlusal views of the maxilla and mandible demonstrating anisognathia.

Left image: Triadan numbering for the maxillary teeth. For deciduous teeth, the first number in the sequence is altered so that the deciduous teeth of the first arcade become the fifth arcade, and the second becomes the sixth.
Right image: Triadan numbering for the mandibular teeth. For deciduous teeth, the third arcade becomes seventh and fourth becomes the eighth.
The Tooth
The equine tooth has a root and a crown. The crown is divided into two portions:
-
Reserve: held within the alveolar socket
-
Clinical: above the gingiva; visible and intraoral.
The root is distinct and forms with age as cementum is deposited apically to the enamel; there is no enamel in the true root section of the teeth, so once the tooth is sufficiently worn, not only is there potential for the root section to suffer an increased rate of wear, but the occlusal surface loses the ability for efficient grinding, as seen in Smooth Mouth. The loss of enamel in particular, results in a loss of texture to the grinding surface and hence the tooth becomes less efficient for mastication with age.
The tissues making up the tooth are the pulp, dentine, enamel and cementum.
The pulp is a soft, gelatinous tissue found within the pulp cavity, horns and canal. The blood vessels, connective tissue and nerves (primarily sensory from the Trigeminal nerve) enter the pulp cavity from the apical foramen.
There is a large common endodontic chamber at eruption; the pulp horns separate with age in the CT, but some pulp horns retain interpulpar communication.
Coronally, the pulp extends as horns (differing in number according to tooth type and location) and apically extends to form root canals.
Variations are:
-
06 cheek teeth: there are 6 pulp horns, with the rostral-most horn numbered 6
-
maxillary 11s: there are 7 pulp horns (caudal-most, numbered 7 and 8)
-
mandibular crowns: the 11s have 6 pulp horns with the caudal-most horn numbered 7
-
remaining cheek teeth: there are 5 pulp horns
-
incisors: there is one common chamber and typically one pulp horn which may split into two branches at the labial border of the infundibula.

A. Rostral
B. Lateral
C. Caudal
D. Holes left from blood supply to cementum
E. Medial
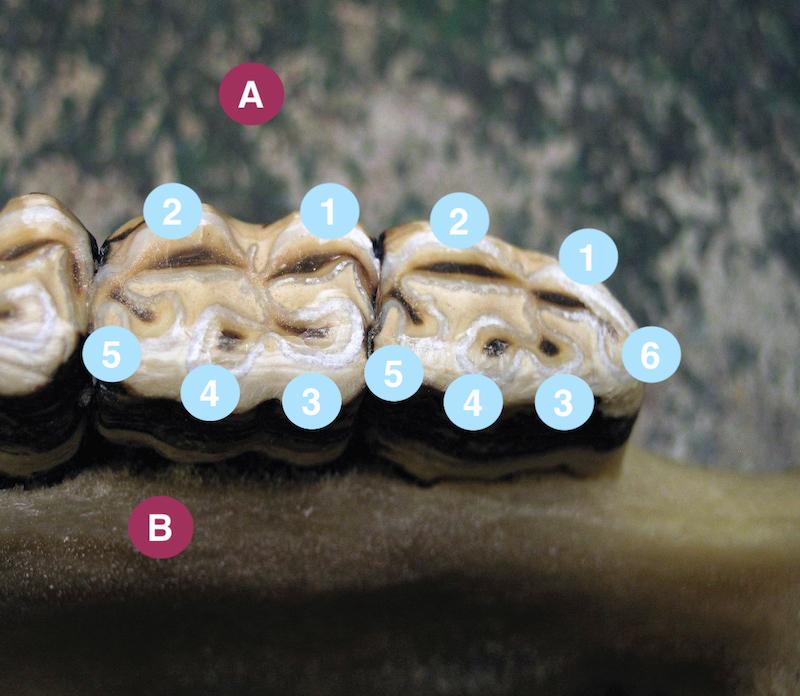
A. Lateral aspect fourth arcade
B. Medial aspect fourth arcade
There is close correlation between the pulp and the dentine:
-
Odontoblasts lay close to the dentine at the peripheral borders of the pulp and are responsible for continuous production of dentine from the extremities of the processes. The processes extend into the circumpulpal aspects of the dentinal tubules and reach the amelodentinal junction and also the occlusal surface, therefore iatrogenic exposure needn’t only be directly from the chewing surface.
-
Cell types include fibroblasts, precursory odontoblasts/fibroblasts (undifferentiated mesenchymal cells; differentiation occurs according to stimulus) and immune cells.
-
Secondary dentine deposition requires a prolonged blood supply throughout life. However, the apical foramina is also subject to deposition of dentine, which causes it to narrow and restrict the diameter of the pulpar blood vessels. With appropriate stimulation, the odontoblasts will continue to produce dentine throughout their life.
The tooth is brittle and there is potential for pulp exposure from a fracture, especially from decalcification disease processes such as caries. Injury can be caused by direct or indirect exposure (iatrogenic via instrumentation or via disease processes initiating crown fracture for example), thermogenesis (as little as an increase of 5.5°C via electromechanical instrumentation), increased pressure leading to anachoresis (may be traumatic i.e. fall or kick), desiccation, and bacterial infection from disease processes (may be pre or post fracture). In human and small animal dentistry, vibratory phenomenon is a threat to pulp inflammation. The risk is increased with lower instrument speeds, often encouraged in equine dentistry to prevent over-reductions, thermogenesis and/or of the plane of rotation in the instrument heads i.e. bearing wear or looseness which also causes unnecessary increases in instrument vibration.
⚠ ALERT
An increase in pulp temperature of 5.5°C can cause irreversible thermal damage.
Dentine is the key supporting component and forms the bulk of the equine tooth. This cream coloured, calcified tissue is apposed by layers of cement and enamel. The hypsodont tooth is effectively laminated, with each dental tissue offering differing rates of wear, resulting in a self-sharpening and undulating surface. The main dentinal structure is the tubule, which projects internally from the outer surfaces to the pulp. Upon dentinal exposure, pain may be transmitted via the circa 25k-58k tubules per mm2.
Dentine may be divided into three core forms, primary, secondary and tertiary/reparative.
Primary dentine forms prior to dental eruption and forms the bulk of the tooth.
Secondary dentine (2D; dark brown at the occlusal surface) is continuous with primary and may be either regular or irregular. The latter was originally thought to be laid in response to noxious stimuli, but its presence is found in apparently unaffected teeth. Irregular dentine is deposited centrally within the pulp horn when in the closing stages of complete pulp replacement by dentine. The depth of the secondary dentine cannot be assumed from the visual appearance of the occlusal surface. Secondary dentine, laid by odontoblasts, compensates for occlusal wear and prevents exposure of pulp. If this sclerotic layer (either calcification of odontoblast processes or the dental smear layer) is removed, sensitive odontoblast processes may be exposed, giving rise to an array of opportunities for necrosis. Occlusally, the secondary dentine should appear almost glassy with no flaws – such as bleeding/leaching of the colour into the primary dentine, holes or fissures.
⚠ ALERT
Crown reductions must be performed visually.
Reduction of the crown requires care; continuing to the point where the occlusal surface is all of a similar cream colour is now considered to be an indirect pulp exposure. Removing the dark stained 2D seal will lead to the leaching of dentinal fluids and migration of odontoblasts (desiccation), which is a painful process and may cause transient negative post-procedural masticative and behavioural changes (quidding, inappetance etc).
Displaced odontoblasts disappear from the tubules via autolysis and are replaced by new cells from the pulp within 1–3 months. For this reason, reductions to overgrown crowns that cannot be reduced to the height of the adjacent ‘normal’ teeth should have subsequent treatment scheduled for 3 months after the initial reduction.
Further reduction to the crown after indirect exposure would result in pink colouration at the 2D site as vital pulp tissue emerges. This pink colouration is a result of direct pulp exposure and warrants immediate treatment by way of pulpotomy, pulpectomy or pulp capping if the tooth’s vitality is to stand any chance of recovery.

Dental tissues of the maxillary cheek tooth.

Dental tissues of the mandibular cheek tooth.
Tertiary dentine may be reparative or reactionary and is deposited as a response from the odontoblasts to noxious stimuli. Newly differentiated odontoblast-like cells are responsible for reparative dentine, while pre-existing odontoblasts lay reactionary dentine.
The enamel is formed by the ameloblasts at the apex of the tooth. The ameloblasts die off once the tooth has erupted and therefore no regeneration of enamel can occur. Enamel is therefore essentially an inert tissue. It is also the hardest substance in the body (96–98% mineral).
It is thought that a contributory factor in maxillary cheek tooth buccal slab fractures is the presence of a greater amount of equine type-1 enamel compared to mandibular cheek teeth where type-2 enamel is dominant.
The CT are highly evolved to be a very efficient start to the digestive process, grinding rough, fibrous ingesta into particles for swallowing. To support this process, the cheek teeth have extensive enamel infolds (particularly the mandibular cheek teeth), which offer increased surface area for effective grinding but also offer laminated style protection to the softer dental tissues.
Infundibula are a normal feature in incisors and maxillary cheek teeth where their length may be around 80% of the total crown length. Each infundibulum may differ considerably in length. Following age-related attrition, one or both infundibulum may erode completely, causing the remaining tissues to wear rapidly beyond the capacity of eruption, and resulting in the tooth becoming concave – a condition known as senile excavation. A similar process may occur in mandibular teeth regarding the enamel infolding, with crowns demonstrating a smooth, almost glass like occlusal surface.
The cementum is the softest of the three calcified dental tissues demonstrating ultrastructural likeness to bone and considered supragingivally inert at the peripheral aspects of the crown. Subgingivally, the cement is very much alive and receives sustenance from the periodontal ligament to its biological cells; the cementoblasts .
Cementum is a specialised calcified connective tissue that provides anchorage for the fibres of the periodontal ligament (Sharpeys Fibres). The continuous deposition of cement allows the attachment of new fibres as the tooth erupts; effectively, the detachment and reattachment of the Sharpeys fibres to new, healthy cement ‘walks’ the tooth in the direction of eruption.
Cementum is also present within normal infundibula (aplasia of which may lead to disease).
Subsequent to eruption, cementum is deposited at the apex of the tooth and this enamel free region is termed the true root.
Peripheral cementum is significantly thicker at the gingival margin than the layer covering the apex. It is deposited both directly and indirectly onto resorbed and unresorbed enamel, with a thin calcified layer interposed in areas of indirect mineralisation.
The periodontium includes all the structures connecting the tooth to the bones of the skull. It plays an important role in eruption and contains blood vessels and nerves. The gingiva, peripheral and apical cement, periodontal ligament and cribriform plate form the periodontium.
The periodontal ligament (PDL) attaches teeth to the alveolar bone via healthy cementum. The PDL has approximately 28,000 fibre bundles mm2; firmly securing the crown yet allowing for minor movement and experience of feel via an array of nerve fibres, blood vessels and collagen bundles (including the Sharpeys fibres). This is one of the reasons that equids rarely chew on stones or other hard materials found in their grazing (dental fractures are usually the result of disease processes). The Sharpeys fibres are embedded within the cementum and aid the facilitation of the eruption process.
The PDL has a well-developed neural and vascular structure with dynamic and regenerative capabilities. In the presence of disease (periodontitis), the PDL and surrounding periodontium may experience significant pain. This can lead to dysmastication, weight loss and performance problems. Disease is common and often results in tooth loss and therefore reduced masticative function.
The compact osseous lining of the tooth socket is known as the alveolar bone and is the radiopaque line surrounding the tooth termed ‘lamina dura’ upon radiography.
The alveolar bone demonstrates a 6 day cycle of formation and resorption which aids remodelling required to ensure the tooth socket reflects the volume of reserve crown accommodated; this is another process that can be utilised for the resolution of periodontal disease.
Below the free margin of the gingiva sits the alveolar crestal bone, which forms the gingival sulcus, but is also useful for evaluation of periodontal disease (although lysis of the alveolar crestal bone may also be a normal consequence of age).
The nerve supply
The dental rows and closely apposed soft tissue transmit sensory information via the Trigeminal nerve (fifth cranial nerve). This exits the skull below the ear and divides into the dorsal Maxillary branch, and ventral Mandibular branch.
-
The Maxillary branch – enters the skull through the Maxillary foramen and runs cranially where it receives nerve branches from each cheek tooth, then exits the skull at the Infraorbital foramen and continues on to innervate the upper incisor teeth.

Infraorbital nerve block site.
-
The Mandibular nerve – lies on the medial side of the mandible and enters the mandible via the Mandibular Foramen where it runs cranially and receives nerve branches from each lower cheek tooth. The nerve exits via the Mental Foramen and continues to innervate the lower incisor teeth.

Mental nerve block site.
DECIDUOUS TEETH AND ERUPTION
Donkeys have similar patterns of eruption to the horse and pony; with some breeds demonstrating significant variance after the adult mouth is complete, making ageing after this time less accurate. Globally, the difference between dental ages of donkey breeds may demonstrate a standard deviation of 12 months, but more commonly, donkeys present as 6–8 months behind horses.

The use of a mirror to visualise the line of demarcation between a deciduous cap and its permanent counterpart.
Table showing typical eruption pattern and timescales in the donkey:
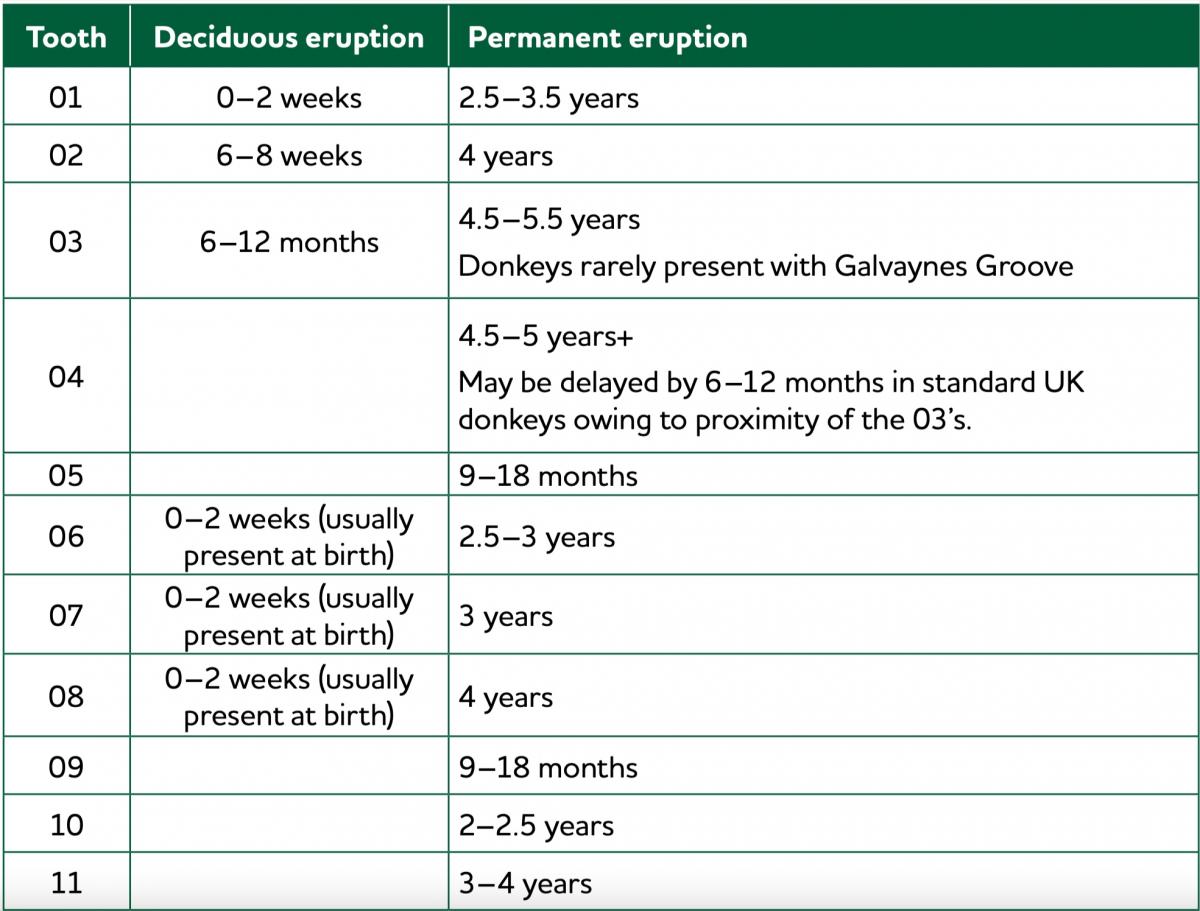
Note: Eruption or permanent teeth in the donkey tends to be 6–8 months later than in horses and ponies.
AGEING THE DONKEY
Ageing equids by the visual appearance of the incisor is typically an educated guess. As more science based evidence arises, it highlights the inaccuracies of ageing by dentition. Factors such as country of residence, species and breed, malocclusions, dental disease, stable vices, grazing masks/ forage containers and quality of feed can have a large effect on incisor wear and therefore decrease the accuracy of age estimation.
Useful points to note are:
- Deciduous incisors are typically very white and much smaller and rounded compared to their permanent counterparts. They should not be easily confused with incisors that have been subjected to a lifetime of wear. If a professional is ever unsure if an animal is juvenile or geriatric and the general demeanour/condition of the animal offers no clues, it is often useful to palpate the mandible and feel for thickness and/or matching pairs of eruption cysts. Thicker mandibles and eruption cysts occur in younger animals. Additionally, when viewed from the lateral side, the angle of the incisors is more vertical in younger equids, becoming more sloping and elongated in older patients.

Larger, squarer and darker permanent central incisors, and smaller, whiter and rounded deciduous 02s and 03s.

Deciduous incisors of a juvenile donkey.
-
The corner incisor may offer a broad indicator of age range; the deciduous corner incisor is lost at approximately 5yrs of age and the permanent erupts into the space available at round 5.5yrs but occlusal contact is not complete across the entire surface. Complete occlusion happens around 6.5–7yrs of age (depending on species and breed), with the presence of a small corner overgrowth of the maxillary 03 at 7–8yrs of age (which reappears in donkeys at approximately 12, 21 and 31yrs). Once the permanent 03 is erupted and in wear;
-
when the tooth is wider than tall, the equid is likely to be under 10yrs of age.
-
when the tooth’s height equals its width, the equid is approximately 10yrs of age.
-
when the tooth is taller than wide, the equid is over 10yrs of age.
-
-
The dental star, which is the secondary dentine protecting the pulp tissue, is visible from around 3.5yrs of age in the central incisors as an elongated line to the labial aspect of the infundibulum.
-
Around 12–15yrs of age the cup or infundibula will begin to gradually disappear from the incisors.
-
By the time the animal is approximately 20yrs of age, the dental stars are circular and more central on the occlusal surface.

Corner incisor of a miniature donkey 6yrs and 2 months old.

Despite being overshot, this 11 year old donkey demonstrates an approximately square corner incisor.

Corner incisor is taller than its width in this 18yr old donkey.

Occlusal view of the mandibular incisors in a 20yr old donkey in Egypt. Note the centralised remnants of the dental star and rectangular appearance of the central crowns. This age related occlusal anatomy differs globally, and between species and their sub types (e.g. donkey, mule or horse; standard, mammoth or miniature).


These donkeys are aged within 2yrs of each other, yet disease processes have had a marked influence over the ability to successfully predict age by dentition.
BIOMECHANICS OF THE ORAL CAVITY
Oral biomechanics is the structure, function and motion of the mechanical aspects of the dental, periodontal and supportive structures including articulations.
Temporomandibular joint (TMJ)
The TMJ is the joint between the articular tubercles of the maxilla and the condylar processes of the mandible and has direct relationships with components of the ear.
It is not uncommon for donkeys with ad lib access to food to masticate up to around 40,000 movements per 24hrs. Of course those with restricted access to foodstuffs, in particular long forage or grass, will perform considerably less masticative movements. It is logical to assume a joint performing in the region of 9–14 million actions per year would be a candidate for degenerative conditions, yet the presentation of TMJ disease in the donkey is rare.
Dental related clinical signs may be causative or symptomatic of TMJ disorders.
Musculature
Relevant muscles are:
-
The paired masseter and temporalis muscles close the oral cavity and perform continuous mastication. It is beneficial during the external examination to palpate these muscles and assess for symmetry. Any asymmetry may divulge useful information regarding mastication and dental disorders.
-
The medial pterygoideus also assists jaw closure; moving the mandible sideways (unilateral contraction) and dorsally (bilateral contraction).
-
The lateral pterygoideus causes the mandible to move medially (unilateral contraction) and rostrally (bilateral contraction).
-
Opening of the jaw is facilitated mainly by the digastricus but is assisted by the occipito mandibularis at the caudal border of the mandible.
-
The muscles of mastication are innervated by the 5th cranial nerve (the mandibular division of the Trigeminal nerve).
Saliva
The production of saliva is stimulated by mastication. It:
-
buffers acids and influences the pH of the upper gastrointestinal tract
-
is distinct from, but continuous with, crevicular fluid
-
has a high pH initially when ejected from the duct; this serves to calcify local plaque. Subsequently, saliva maintains a reduced pH; this is why calculus deposits more commonly occur at teeth local to salivary ducts
-
varies pH according to the ingesta; concentrate feed will reduce the salivary pH and forage matter will increase the pH. This will affect the buffering capacity in the stomach, but the pH will return to a base value post feeding of circa 8.7; which is the same value seen when eating hay or fresh grass
-
aids taste
-
washes non-adherent bacteria and debris from tooth surfaces
-
is composed primarily of water, but contains sodium, chloride, sodium bicarbonate, lactoperoxidase and immunoglobulin A (giving antibacterial properties)
-
lubricates and protects oral tissues; facilitates transfer of ingesta to the stomach
-
increases in volume if disease is present.
⚠ ALERT
Hypersalivation may be an indicator of a dental disorder.
The parotid is the largest salivary gland and is found at the retromandibular fossa; the caudal border of the ramus, extending down from the base of the ear. The ducts empty at approximately the level of 1 and 207/8 and care must be taken whilst performing equilibration not to cause injury to this area. Donkeys and older equids may present with extensive calculus around the premolars due to the proximity of the duct.

Enlarged sublingual tissue.
The mandibular ducts can be found under the rostral aspect of the tongue and polystomatic submandibular tissue is found at the ventrolateral aspects of the tongue.
Mastication
Important points to note are:
-
Anisognathia in donkeys is 30% compared to horses at 23%. The difference is thought to stem from a narrower mandible.
-
The average occlusal angle of CT is roughly 12–15° but this is not consistent over the length of the entire dental row (steeper caudally, but 10–20° is normal in the same CT row).
-
The length of CT rows should be approximately equal.
-
Mastication may be affected by the type of ingesta, dental/oral pain, disease, trauma, congenital abnormalities including conformation, and primary and secondary influences (including iatrogenesis) and malocclusions.
The velocity of masticative stroke occurs at the premolars and compression occurs at the molars. While it may be reasonably assumed equids may therefore cope well with the complete absence of premolars; those with multiple tooth loss at randomised locations throughout the complete arcades generally have a higher longevity than those with multiple tooth loss in adjacent teeth (i.e. all of the molars or premolars, or even a complete arcade).
The angulation and corrugation of the CT and the range of motion of the mandible together with the proximity and interaction with the tongue will help to grind and rotate the ingesta whilst spiralling the bolus towards the throat for deglutition. The three stages of mastication are widely featured in other texts.
The aim of mastication is to reduce feedstuffs to an optimal fibre length for digestion. The efficiency of this process may be assessed by observation of the faecal fibre length. The optimal faecal fibre length for donkeys is just short of 2mm.
⚠ ALERT
Average faecal fibre lengths of over 3.6mm are indicative of dental disease and faecal fibre lengths over 4.5mm are indicative of severe dental disease.
Faecal fibre length may be of use when monitoring quality of life.
See chapter 9. Nutrition of the Donkey with Dental Disorders for more information on feeding donkeys with dental disease.
When the incisors are at neutral there is no occlusal contact in the CT in the normal mouth. Occlusion only occurs during lateral excursion of the mandible. Deliberate manual lateral excursion of the mandible is therefore a useful biomechanical indicator. All CT within the row performing active mastication should make contact at a similar time. The point at which the incisor teeth separate is the point at which the cheek teeth are in contact. Occlusion may be observed by retracting the cheek and assessing for equal and uniform apposition along the entire arcade.
A longer period of lateral excursion before incisor separation indicates reduced CT occlusion. Incisors that separate markedly, dorsally and/or immediately may indicate cheek tooth abnormalities and/or pain (shear mouth, overgrowths, fractures). When assessing lateral excursion, it is important to assess both sides; cheek tooth pathology may be correlated to restricted lateral movement or premature incisor separation at the affected side.
Effect of malocclusions on mastication
To a certain extent, equids are able to be selective in how the CT occlude. They will adapt mastication to relieve areas which may experience pain. As a result these crowns usually receive less wear and may become overgrown and/or extremely sharp.
Where dental overgrowth is present, the dominant crowns may encourage the formation of diastemata at the mesial and/or distal interproximal spaces; this happens through mechanical separation of the crown during chewing.
Masticative forces play a role in the attrition of dental crowns and, therefore, the rates of compensatory eruption. The periodontal ligament is designed to withstand a range of forces; forces outside of the upper range are encouraging of pathological response, potentially leading to ankyloses.
The rate of wear is increased in younger animals when the dentinal tubules are hollow and the crowns not so resilient to attrition; the eruption rate is therefore equally increased. As the animal ages, eruption slows in line with the wear rate and may even cease altogether in the presence of ankyloses. Wear rate will eventually exceed eruption when there is insufficient reserve crown to compensate for crown loss.
⚠ ALERT
Equilibration must allow the patient to regain and maintain occlusion following crown reduction.
This is an important physiological process to be mindful of when performing dental reductions in older animals.

About
How to reference this publication (Harvard system)?
(2021) “Clinical Anatomy”, The Clinical Companion of Donkey Dentistry. Available at: https://www.ivis.org/library/clinical-companion-of-donkey-dentistry/clinical-anatomy (Accessed: 19 May 2024).
Affiliation of the authors at the time of publication
Sidmouth, Devon, EX10 0NU
Author(s)
Copyright Statement
© All text and images in this publication are copyright protected and cannot be reproduced or copied in any way.Buy this book
Buy this book
The Clinical Companion of Donkey Dentistry is an easy reference book for professionals produced as part of a series of specialist books that will compliment The Clinical Companion of the Donkey. It enables us to share our vast knowledge and experience to improve the health and welfare of donkeys globally.
Following on from the publication of The Clinical Companion of the Donkey, we plan to produce a series of in-depth specialist handbooks which will complement the handbook.
This book is intended as a guide to the anatomical features of the head and oral cavity of the donkey, to offer a greater understanding of the oral and dental disorders that may affect these animals throughout their life, and how to correctly examine, diagnose, prevent and/or treat pathological situations.
Dentistry is the first topic to be published in this series, and we consider it to be an area which is extremely important to the health and welfare of donkeys globally, while being misunderstood and undervalued by many communities.
This book allows us to share our vast knowledge and experience in donkey specific dentistry and has been produced as an easy reference and well-illustrated book, which we believe will not only increase awareness, but also the confidence of professionals in carrying out dental care and treatment in donkeys.
Comments (0)
Ask the author
0 comments