
Acute Desmitis of the Accessory Ligament of the Superficial Digital Flexor Tendon (Proximal Check Ligament) in 26 Thoroughbred Race Horses: Clinical Features and Prognosis for Racing
J. M. Reimer
Read
Abstract
Spontaneous injury of the accessory ligament of the superficial digital flexor tendon (AL-SDFT) may be an important and underdiagnosed condition in the Thoroughbred racehorse. Although effusion within the carpal canal is an easily recognized feature in some cases, it is not present in all cases: Subcutaneous (SC) thickening over the proximal aspect of the palmar metacarpal region and of the palmar-medial carpal region may be the only clinical findings at the time of examination. Recognition of the condition and appropriate rehabilitation provide a very good prognosis for return to racing.
1. Introduction
Ultrasonographic diagnosis of injuries to the accessory ligament of the superficial digital flexor tendon (AL-SDFT) has been described [1,2]. Injury of the AL-SDFT is mentioned infrequently in the literature [1-4]. The condition has been described in a group of racehorses, sport horses, and pleasure horses, with follow-up information available on approximately 65% of cases [1]. Injury of the AL-SDFT was often accompanied by other abnormalities, including synovitis, tendonitis, and proximal suspensory desmitis [1]. Prognosis for this injury has been described as being fair, with treatment consisting of intrathecal hyaluronic acid and corticosteroids, and restricted and controlled exercise for up to 6 mo [3]. The purpose of this paper is to describe the clinical features of AL-SDFT injury in Thoroughbred racehorses and the prognosis for racing.
2. Materials and Methods
Ultrasound records of all horses, in which a diagnosis of acute AL-SDFT injury was made by the author, were reviewed. The signalment, history, clinical findings, and sonographic findings were recorded. Ultrasound images were obtained with a 7.5-MHz transducer; a stand-off was generally not necessary. Short- and long-axis images of the AL-SDFT were obtained from the level of the distal chestnut to the level of the radiocarpal joint at the medial aspect of the distal forelimb as described by Denoix and Busoni [2]. A diagnosis of AL-SDFT injury was made based on a diffuse decrease in echogenicity and hypoechoic appearance to the ligament or a discreet area of fiber tearing. Long-axis views showed marked loss of fiber alignment as well. The opposite AL-SDFT was always imaged to better illustrate the anatomy and abnormalities. The superficial digital flexor tendon (SDFT), deep digital flexor tendon (DDFT), proximal inferior check ligament, proximal portion of the suspensory ligament, and carpal canal fluid and synovium were always examined as part of the study. Ultrasound images were recorded on thermal print paper.
Race records of affected Thoroughbreds were obtained from the Jockey Club's Information System, and the time from known date of injury or diagnosis to subsequent race was calculated. The median of the average earnings per start were compared before and after treatment for those horses that returned to racing. Average earnings per start were calculated for each horse using no more than the five preinjury races and no more than five post-injury races. Followup information for horses that did not return to racing was obtained by contact with the owner.
3. Results
Twenty-seven horses were diagnosed with acute AL-SDFT injury. Twenty-six horses were Thoroughbreds, and one horse was an American Saddle horse. The Thoroughbred horses were included in the study for further analysis.
There was one 2-yr-old horse, seven 3-yr-old horses, and 18 horses 4 yr of age or older. The right forelimb was involved in 18 horses, and the left involved in 7 horses. One horse suffered a left fore injury and 16 mo later suffered a right fore injury during his first return to race.
Clinical history included transient lameness (8 cases), persistent effusion of the carpal sheath (12 cases), recurrent effusion of the carpal sheath (4 cases), and/or apparent thickening of the proximal SDFT mimicking the clinical appearance of a "bowed tendon" (13 cases). In all cases, palpation of the medipalmar carpal region revealed thickening compared with the opposite limb at the time of the ultrasound examination.
Ultrasonographic findings revealed an enlarged hypoechoic AL-SDFT with poor fiber alignment in the majority of cases (Fig. 1 and Fig. 2). Seromas or discreet areas of tearing within the AL-SDFT were found in four cases, one case in which a poorly healing injury was exacerbated when the horse ran off with the rider. Additional ultrasound findings included peritendinous thickening over the SDFT in the proximal palmar metacarpal region (13 cases) and/or variable degrees of effusion within the distal aspect of the carpal canal. Fluid within this region of the carpal canal ranged from no appreciable fluid (3 cases), mild effusion (7 cases), and moderate effusion (the distance between the DDFT and the inferior check ligament was 0.5 cm or greater [13 cases]) to marked effusion (fluid depth greater than 0.5 cm accompanied by flattening of the inferior check ligament and/or effusion within the carpal canal proximal to the level of the accessory carpal bone [4 cases]). Abnormalities of other structures within the limits of the carpal canal were infrequent but included mild decrease in echogenicity of the origin of the suspensory ligament (four cases), mild decrease in echogenicity of the SDFT (one case), chronic bowed SDFT (one case), and mild synovial thickening of the carpal sheath (one case).
Figure 1. Short-axis image of the superior check ligaments in a horse with a left-sided injury. The left side of the image illustrates a diffusely hypoechoic left superior check ligament compared with the normal echodense right superior check ligament (right side of image).
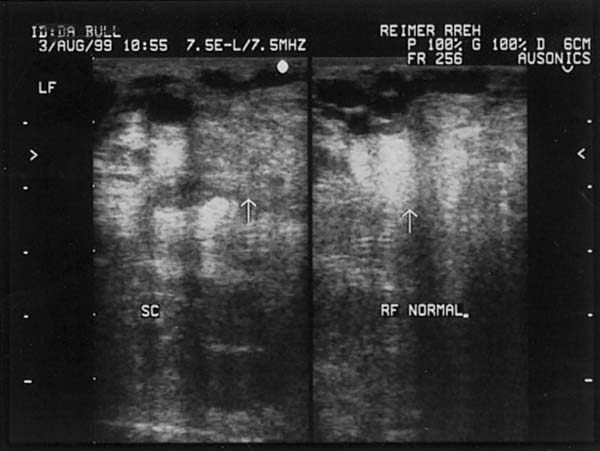
Figure 2. Long-axis image of the superior check ligaments in the horse described in Figure. 1. Notice the hypoechoic appearance and loss of fiber alignment in the abnormal ligament (left side of image) compared with the normal ligament (right side of image).

Recommendations generally included 4 - 8 wk of stall rest with hand or tack walking, followed by 4 - 8 wk of turnout, and finally, a gradual return to training.
Repeat ultrasound examinations were performed in 11 horses. Eight horses had improvement in the sonographic appearance of the AL-SDFT characterized by return or near return to normal size and echogenicity, but with nonparallel fibers. One horse that appeared well-healed after 2.5 mo began swimming and suffered exacerbation of the injury. After 2 mo of walking, the ligament returned to near-normal appearance. Another horse, being exercised on a water treadmill, had deteriorated at 2 mo post-injury, and recommendations were made to discontinue the water exercise. Swimming was used for rehabilitation of a third horse, who had very poor healing of the ligament at 5 mo postinjury. Recommendations were made to discontinue swimming and jog the horse; however, the horse ran off with the rider and exacerbated the injury. After 3 mo of walking and stall rest, the ligament appeared nearly normal. One horse had deterioration of the injury after 2 wk of jogging preceded by 4 wk of stall rest and hand walking.
Four horses are currently in rehabilitation or are in training as of this writing. Two previously successful racehorses were retired for breeding, and one unraced 4-yr old horse was retired on diagnosis. One horse had successfully returned to training but died before returning to race. Of the remaining 18 horses, 17 (89%) ultimately returned to racing. One horse failed to finish when he injured the opposite AL-SDFT at his first return to racing 16 mo after the injury; however, he subsequently returned to racing 6 mo later. The mean and median times to return to racing were 8 and 7.5 mo, respectively (range: 2 wk - 16 mo). Aside from the horse that failed to finish at his first return to racing, that individual and 2 others ultimately completed three starts, 3 horses completed four starts, and 11 horses completed five or more starts. The median of the average earnings per start within five starts before the injury was $3686, whereas the median of the average earnings per start for up to five starts after the return to racing was $719.
4. Discussion
Acute desmitis of the AL-SDFT may be an underdiagnosed condition in the Thoroughbred racehorse. Since becoming aware of this condition and the ultrasonographic technique for diagnosis, the author has diagnosed 27 cases through our practice in a little over 7 yr. Two individuals in this study were pulled up during Breeder's Cup races, emphasizing the importance of this injury. It was interesting to note the predominance of the Thoroughbred racehorses and absence of the Standardbred racehorses in this study. European trotters are more commonly affected by this condition, while it seems to be rare in North American trotters [3]. Also of interest is the preponderance of the injury in racehorses 4 yr of age and older, the tendency to involve the right forelimb, and the absence of other pathology in the carpal canal region. This is in contrast to the study reported by Denoix et al., [1] in which younger individuals were affected and pathology of additional structures of the carpal canal region were diagnosed.
A history of transient lameness and/or carpal sheath effusion should alert the clinician to the possibility of AL-SDFT injury [1,3]; however, it was found in this study that the presence of peritendinous edema in the proximal metacarpal region, mimicking the appearance of a bowed tendon, may be the only complaint and should prompt examination of the AL-SDFT. Palpable thickening of the tissues in the palmar medial carpal region seems to be a fairly consistent finding in the author's experience.
Swimming or water treadmill exercise seemed to be detrimental to AL-SDFT injury, even when initiated after 2 mo of conservative management. Injection of the carpal sheath with hyaluronic acid and/or corticosteroids was not performed in the horses in this study to our knowledge. Recommendations for management of this condition in this group of horses were to provide 4 wk of stall rest and hand walking, followed by 4 wk of small paddock turn out or 8 wk of stall rest with hand walking followed by a gradual return to training. Repeat ultrasound examination is recommended at 2 mo post-injury. If the ligament seems of uniform and normal echogenicity, jogging may resume with anticipated return to racing as early as 6 mo post-injury in some cases.

Comments (0)
Ask the author
0 comments