
The Equine Foot - Form and Function
Author(s):
S.E. O’Grady
In: AAEP Focus Meeting - Focus on the Foot - Fort Collins, 2013 by American Association of Equine Practitioners
Updated:
SEP 07, 2013
Languages:
Read
I. Introduction
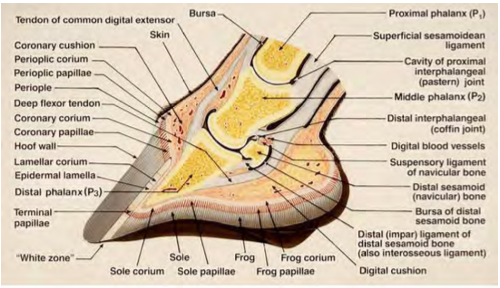
THE foot is interesting and unique as it is a group of biological structures that follows the laws of biomechanics (Fig. 1). It is also the authors’ opinion that the foot is also the dominant site of lameness in performance horses. Therefore, every time farriery is performed on a horses’ foot, the form and function of the foot will be affected. The digit is that part of the limb distal to the metacarpophalangeal joint. The foot is the part of the distal limb encased by the hoof. The hoof (ungula) is, by definition, the integument or skin of the foot. The hoof capsule is formed by the cornified layer of the epidermis in the various regions of the hoof.
Fig 1. Schematic illustration showing the biological structures of the foot along with the biomechanical properties focused at the distal interphalangeal joint. Courtesy of Dr Chris Pollitt.
II. Form
The gross morphologic differences between the distal limb and the rest of the musculoskeletal system cause some intimidation. However, to overview the distal limb as a cause of lameness, there are only so many structures in the foot and there are only so many pathological processes that may occur in each structure. The acronym ‘DAMNIT’ which stands for degenerative, anomalous, autoimmune, metabolic, nutritional, neoplastic, inflammatory, infectious, and traumatic could be used to demonstrate this concept. By understanding how these structures function normally and considering all the potential processes that may occur, a specific diagnosis may become more readily apparent or the diagnostic puzzle can be reduced through the process of elimination. Furthermore, a thorough knowledge of foot anatomy and the associated biomechanics provides concise guidelines for applying the appropriate farriery to any given foot. These guidelines can be used to maintain the health of the foot or can be applied to address a pathological process.1-3
The proximal and middle phalanges are structurally unremarkable compared to the long bones of the limb. They are flattened cylinders, more so palmar/plantar than dorsally with well-demarcated cortices and medullary cavities. The distal phalanx however is unique. It has three surfaces: the articular surface, the parietal surface and the solar surface. The parietal surface forms a large surface area that is porous and roughened – ideally adapted for a broad attachment to soft tissue and to allow vessels to penetrate.
The solar surface is hard and smooth with no vascular foramina. Attached to the palmar process of the distal phalanx are the collateral (ungual) cartilages. These cartilages are flat rhomboid plates in a shape that extend proximally from the palmar process so that approximately 50% of each cartilage is proximal to the coronary band. The ungual cartilages could be thought of as an extension of the distal phalanx. Both interphalangeal joints are saddle joints such that motion is primarily restricted to extension and flexion in the sagittal plane but this configuration also allows considerable counter-rotation in the frontal plane. The distal interphalangeal joint has a much greater range of motion than the proximal interphalangeal joint. The distal interphalangeal joint has three separate articulations: 1) between the middle and distal phalanges, 2) between the middle phalanx and the distal sesamoid bone, and 3) between the distal phalanx and the navicular bone. There is very little movement between the distal phalanx and the distal sesamoid, so they are frequently treated as one unit and should be considered as moving together.4
The articular surfaces of the phalanges of both interphalangeal joints are maintained in apposition by paired collateral ligaments. In the proximal interphalangeal joint, the palmar aspect of the joint is supported by the proximal scutum and the flexor tendons along with and 2 pairs of abaxial and axial palmar ligaments. In the distal interphalangeal joint, the position of the distal sesamoid bone is stabilized and held in place by the paired collateral ligaments of the distal sesamoid proximally and the impar ligament distally (Fig. 2). The wide expanse of the deep digital flexor tendon supports the distal interphalangeal joint palmarly (Fig. 3). In addition to these ligaments, there are 5 small ligaments and peri ligamentous/ tendinous fibers associated with each ungual cartilage.
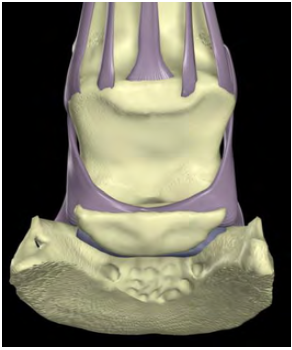
Fig. 2 shows the two pairs of palmar ligaments that span the proximal interphalangeal joint and the three ligaments that maintain the position of the navicular bone in relation to the distal interphalangeal joint.
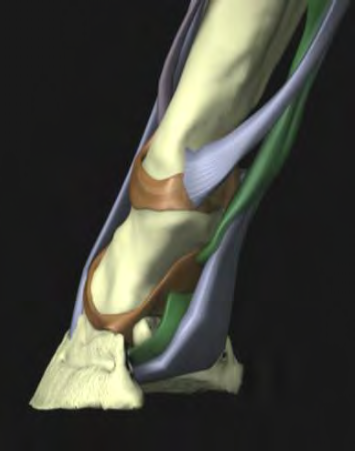
Fig. 3 shows the wide expanse of the deep digital flexor tendon. The tendon forms a sling into which the distal phalanx descends during weight bearing which will function as a shock absorbing mechanism. Its functionality will be base on the integrity of the structures in the heels of the hoof capsule.
It is the integument of the foot that really separates the foot apart from the rest of the musculoskeletal system.3 Like the skin, the integument of the foot (hoof) is composed of 3 principle layers: epidermis, dermis (corium), and subcutaneous tissue. Like the skin, the epidermis is further subdivided into layers: the stratum basale and the stratum spinosum, which are collectively known as the stratum germinativum, and the stratum corneum. The stratum corneum forms the hoof capsule.
Unlike the skin, which is relatively uniform over the surface of the body, the hoof can be divided into 5 distinct regions based on their gross appearance: coronary band, wall, sole, frog and heel bulbs. Underlying the hoof, the germinal layers of the epidermis, the dermis and the subcutaneous tissues are highly specialized and are named after the tissues they generate or support: perioplic (limbic), coronary, lamellar, solar and cuneate (frog). The terms used to describe the region and epithelial types are not necessarily interchangeable because the surface does not necessarily reflect the type of underlying epithelium.
The limbus or periople is a narrow band of modified skin that bridges the gap between the skin of the pastern and the coronary band, and forms the stratum externum of the hoof wall. The corona is the band like proximal segment of the hoof frequently called the coronary band. The coronal subcutaneous tissue forms the coronary cushion, the coronal dermis follows the curve of the coronary cushion from which the dermal papillae project and the germinal layers of the coronary epithelium, which follow the contour of the dermal papillae, generate the tubular and intertubular horn of the stratum medium of the hoof capsule.
The laminar integument covers the parietal surface of the distal phalanx and the ungual (collateral) cartilages. The laminar subcutaneous tissue forms the modified periosteum or perichondrium that covers the distal phalanx and ungual cartilages. The lamellar dermis forms the primary and secondary ridges that run in a proximal to distal direction to form lamellae that interdigitate with the epidermal lamellae. The primary epidermal lamellae are keratinized, the secondary lamellae are not. The lamellar epidermis forms the stratum internum of the hoof wall. The solar integument covers the solar surface of the distal phalanx. The subcutaneous tissue likewise forms the modified periosteum of the solar surface of the distal phalanx, the dermis forms the dermal papillae and the overlying epithelium forms the tubular and intertubular horn of the sole. [...]
About
Copyright Statement
© All text and images in this publication are copyright protected and cannot be reproduced or copied in any way.Provided by:

Comments (0)
Ask the author
0 comments