Racetrack Emergencies: So What's the Worst That Could Happen?
Read
1. Introduction
Effective management of racetrack emergencies is initiated before the first horse sets foot on the track. The veterinarian should attempt to identify potential emergencies and develop a plan to address them before they occur. Although each event is unique, it is far easier to modify an existing plan than to develop a plan in the middle of the emotionally charged environment that surrounds a racing emergency.
Before serving at a racing event, the veterinarian should (1) understand the nature and relative frequency of race-related musculoskeletal injuries or emergencies that may arise and identify any risks inherent to the specific facility; (2) assess available resources for management of emergencies; and (3) be proficient in the physical and/or chemical restraint of injured horses, rapid clinical assessment, application of external stabilization devices, and the loading and transport of injured horses.
2. Racing Injuries
Ninety-five percent of race-related fatalities are attributed to musculoskeletal injury [1]. Catastrophic injuries sustained by the Thoroughbred race horse occur predominantly in the metacarpophalangeal joint and associated structures of the forelimb [2].
Figure 1 displays incident occurrence over two race meetings and identifies the location on the track where race-related incidents were addressed [a]. It defines the area from the beginning of the final turn to the finish wire as having the highest occurrence of catastrophic injuries and permits staging of emergency resources to provide rapid response to the most severe injuries.

Figure 1. On-track distribution of race-related veterinary emergencies.
In addition to race-related musculoskeletal injuries, other emergencies may include trauma-related injuries (which can occur at any location from paddock to winner's circle), exhaustion, postexertional distress, or collapse and sudden death. The veterinarian should be mindful that on-track emergencies can occur after the race. Veterinary responsibility extends until such time as all horses have exited the racetrack.
3. Resources
Personnel
It is uncommon that a racing injury is managed by a single individual. Therefore, it is important to have an understanding of the skill level of individuals assisting in the management of an emergency. The veterinarian is responsible for maintaining a safe working environment and, to that end, must be prepared to direct the activities of laypersons on scene. For personnel identified as likely to be assisting with emergency care, basic training in equine restraint and human safety is beneficial.
The equine ambulance driver must be proficient in maneuvering the unit. If time permits, it is recommended to schedule mock ambulance deployments that require specific ambulance placement as for a non-ambulatory or severely compromised horse. These drills also serve to identify areas that are poorly accessible or inaccessible by the equine ambulance and allow for the development of a plan for transport of injured horses from those locations.
Although owners, trainers, or stable employees may be present, it is preferable to have a trained assistant responsible for restraint of an injured horse. It is critical that the responsible individual be objectively focused on restraining the horse both to prevent further injury to the horse and to maintain the safety of persons addressing the injury.
Security personnel may be required for crowd control, management of non-participants, and/or media containment. Recognize that these individuals may not have equine experience and will likely require specific direction from the veterinarian on scene.
The on-track veterinarian must also determine the availability of practicing veterinarians to receive cases-both on and off site. It is helpful for racetrack management to establish a policy requiring each veterinary practice to be represented on site when clients' horses race. A list of veterinarians' and trainers' cell phone numbers is carried by the on-track veterinarian and permits discreet, direct notification of initial assessment and facilitates case transfer. The patient remains the responsibility of the on-track veterinarian until case transfer to the attending veterinarian.
Materials, Equipment, and Supplies
The equine ambulance should be a modified, fully enclosed two-horse trailer with both rear and side loading capabilities. A hydraulic floor will facilitate the loading of injured horses and is necessary for loading downed or deceased animals (Fig. 2). If the floor is fixed, alternate humane arrangements must be secured for transporting recumbent horses. Flooring should be a non-porous, non-slip surface.
A partition should transect the front area, providing a barrier between the injured horse and its handlers (Fig. 3a). A moveable middle partition is useful for supporting unsteady patients (Fig. 3b). The Kimzey equine ambulance [b] is equipped with these features and is commercially available.

Figure 2. Ambulance in lowered position.
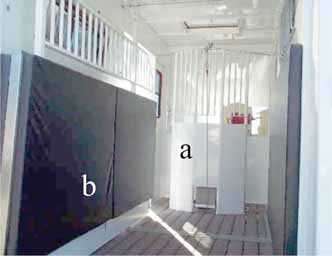
Figure 3. Ambulance interior.
For the transport of recumbent or deceased horses, the ambulance should be equipped with a winch and mat or rescue sled to which the winch cable can be attached. Encircling a dead horse's neck or extremities with the cable is to be avoided in public view.
A tarp or other portable barrier should be carried and used in the event a horse must be euthanized on track. The barrier may be "hinged" by attaching a rigid vertical support in the center to create a treatment area screened from several viewing angles.
When warranted by weather conditions, supplies for facilitated cooling-ice, water, buckets, sponges, and sweat scrapers-should be carried in the ambulance.
If medications are to be carried in the ambulance, a secure lock box should be installed.
External stabilization devices range from commercially engineered products to simple, homemade splints. If sufficient consideration is given to the stabilization requirements of different types of injuries, PVC pipe, rake handles, or broomsticks can be used in the construction of appropriate, functional splints.
The Kimzey Leg Saver [c] splint is available in two lengths. The standard splint, extending to the level of the proximal MC3, is appropriate for injuries to the suspensory apparatus clinically manifesting as hyperextension of the fetlock. The long splint is applied in cases of carpal joint hyperextension; however, a Robert Jones bandage is equally suitable. In the author's experience, the long splint must be slightly bent for a horse to be sufficiently ambulatory to load into the ambulance. (The manufacturer provides instructions for splint modification.) Neither Leg Saver splint alone is appropriate when mediolateral instability is present.
Store Leg Saver splints ready-to-use with the straps rolled up rather than wrapped around the metal shaft of the splint (Fig. 4). Use extreme care when applying the splint, because a fractious horse and a partially applied splint can result in a potentially dangerous situation. The veterinarian may elect to wrap the affected limb before application of the splint; however, excessive padding may allow the splint to shift or loosen.

Figure 4. Kimzey Leg Saver Splint.
Hinged compression boots are useful for stabilizing forelimb P1 and/or P2 fractures, condylar fractures, or fetlock instability in one or more planes (Fig. 5a). An inventory of several sizes is required because fit is crucial for stabilization. It is the author's preference to replace ski-boot latches with Velcro straps for ease of application and adjustment of fit (Fig. 5b). Additional padding in the form of leg cottons or quilts may be necessary to achieve correct fit.

Figure 5. Compression boot.
Stabilization of distal hindlimb fractures is more challenging because the injured horse will typically attempt to "shake off" any device applied. The majority of these horses are non-weight bearing while remaining functionally ambulatory. If necessary, these horses may be loaded, squeezed, and transported to a setting where a veterinary team can apply injury appropriate stabilization under a controlled setting.
In the absence of a confirmed diagnosis, the application of a splint is based on clinical impression. The limitations of an initial on-track assessment are obvious. As an example, all of the fractures shown in Fig. 6 may have the same clinical presentation on track.
Figure 6. Examples of fracture injuries with similar clinical presentation.
For injury A, external stabilization may be unnecessary, but application of either the Leg Saver or a compression boot is not inappropriate.
Injury B may be destabilized by the application of either the Leg Saver or compression boot because both can result in a fulcrum at proximal MC3.
Injury C requires no stabilization, and clinical response to the application of the Leg Saver may be poor because the splint puts direct pressure on the fracture.
For injury D, the application of a compression boot may be preferable to the Leg Saver splint, but either is acceptable.
Recognizing the range of injuries that may have a similar clinical presentation, in the absence of a preliminary diagnosis, it may be appropriate to sedate, load, and "squeeze" the horse without the application of external stabilization.
Under no circumstances is it appropriate to apply an antiphlogistine wrap, Cool Cast [d] as a fracture stabilization device.
It is important that adequate physical and/or chemical restraint be used even when the limb seems to be stabilized. Be mindful that with the application of any splint, the horse has been effectively armed.
Additional supplies include a 20-to 30-ft length of rope (to be used for tail tie or rolling a down horse) halter, lead shank, towels (may serve as blindfold), buckets, sponges, sweat scrapers, ice, rubbing alcohol, sterile bandage material, leg cottons, vetwrap, exam gloves, and duct tape. Hand sanitizer or antiseptic hand wipes should be carried and used between patient contacts.
The veterinarian's emergency medical bag should contain needles, syringes, euthanasia solutions, sedatives, analgesics, and short-acting corticosteroids. Euthanasia supplies should be kept segregated from other medications. It is recommended to have a dose of euthanasia solution pre-loaded to avoid unnecessary delay should on-track euthanasia be required. Euthanasia solutions are controlled substances and must be stored and administered and use must be recorded according to DEA regulations.
The decision to carry and administer non-steroidal anti-inflammatory drugs (NSAIDs) on track should be made in consultation with practicing veterinarians.
Additional supplies to consider carrying include binoculars, alcohol-based hand sanitizer, a blood sampling kit, and a digital camera.
4. Restraint
There is no equine injury that justifies the generation of a human injury.
It is critical for human and equine safety that the patient be adequately restrained. When possible, avoid delegating restraint of an injured horse to an individual directly connected with the horse. A strong emotional reaction to an equine injury can override common sense and create an unsafe environment for all present.
Physical Restraint
Always have the handler stand on the side of the non-injured leg. Be alert to the potential arc of flight that an injured extremity or flail limb could take. NEVER have the attendant stand directly in front of the horse. Attendants of a down horse should work adjacent to the spine, never between the legs or between the head and the forelegs. The veterinarian should remain alert to the location of persons present both for their safety and to afford the veterinarian an escape route. Persons not directly involved in injury management should be directed to stand well removed from the injured horse and its attendants.
Before the administration of chemical restraint, the positioning of an outrider's mount near the injured horse may provide a calming effect on an anxious horse.
Chemical restraint is preferable to the use of a twitch, which poses human safety concerns when applied in the confines of the horse ambulance and negative public perception when used outside the ambulance.
Chemical Restraint
Xylazine [e], administered immediately after exercise at 2.2 mg/kg, IV, is both safe and reliable [3] A standard dose of 1.1 mg/kg is not sufficient to effect sedation. It is important to remind handlers that horses having been administered xylazine retain the unimpaired ability to kick, even if non-weight bearing on a forelimb. Alternatively, sedation after exercise may be achieved by the administration of detomidine [f] at 40 μg/kg, IV.
General anesthesia may be induced with detomidine (40 μg/kg, IV) followed at 5 min by tiletamine/ zolazepam [g] (1 mg/kg, IV). Greene et al. [4]. showed that duration of anesthesia was adequate for patient loading, transport, and transfer to inhalation anesthesia, a procedure requiring ~15 min. Success of this protocol requires a coordinated effort between the on-track veterinarian and the recipient facility on or off site. For transport of patients to an off-site facility, consider the "worst case scenario" with respect to traffic congestion. The transport of an anesthetized horse should not be first attempted in response to an actual emergency.
5. Communication
Promptly communicate with racing officials regarding emergency case management. It may be necessary to delay deployment of track maintenance equipment or the next race's entrance on the track pending the stabilization and transport of an injured horse. When communicating by two-way radio, avoid transmitting detailed information because multiple racing officials and track employees may use a shared radio channel.
The case must be effectively transferred to the receiving veterinarian, and until this has been accomplished, the patient remains the responsibility of the on-track veterinarian. Information regarding initial assessment and any medications administered should be communicated directly between veterinarians.
After having addressed the immediate health needs of the injured horse, the attending veterinarian should communicate calmly, professionally, and honestly with concerned individuals. Specific injury information should be provided only to the owner, trainer, and/or attending veterinarian. Confirm the identity of individuals seeking information before releasing specific details of an injury and its outcome. This is of particular importance with phone requests, and it is appropriate to decline to release confidential medical information over the phone if the identity of the caller is unclear. Although it may be appropriate to speculate to the owner/trainer/veterinarian regarding the nature of the injury-"I'm concerned we may be dealing with a pelvic fracture,"-it is not appropriate to do so with either the media or public requests for information. "The horse was showing signs of left hindlimb lameness after finishing the race. A more comprehensive examination will be performed to determine the cause of the lameness".
Media presence must not interfere with the treatment of an injured horse. Media requests for information, in the absence of an AAEP On-Call Veterinarian, are often directed to the on-track veterinarian. It is appropriate to defer responding to any questions until the case has been transferred to the receiving veterinarian. If the veterinarian is unfamiliar with the individual making an information request, it is appropriate to refer them to the racetrack's publicity/media director.
6. Specific Considerations
There is no guarantee that only one emergency will occur at a time. Be prepared for multiple incidents.
Ataxic Horse
Differential diagnoses include myositis, exhaustion, pelvic or femoral fracture(s), and spinal cord trauma. Because pelvic and/or femoral fractures are associated with significant internal hemorrhage, sedation may further compromise this horse. It is appropriate to administer prednisolone sodium succinate [h] (500 mg, IV) and proceed with physical restraint. Transport the patient by equine ambulance with the moveable center partition adjusted to stabilize the horse. The additional use of a tail tie may be warranted for horses showing severe hindlimb ataxia. Attendants should be safely positioned in front of the partition because hypovolemic shock may result in the abrupt collapse of the horse. It is recommended that an ataxic horse not be off loaded from the equine ambulance until the receiving veterinarian is present.
Recumbent Horse
Differential diagnoses include exhaustion, vertebral and/or pelvic fracture, spinal cord trauma, multiple limb fractures, fracture of a single "down" leg, aneurysm, cardiac failure, and exercise-induced pulmonary hemorrhage. Physical restraint of a recumbent horse should not be overlooked; the veterinarian's assistant is positioned at the horse's poll to maintain the horse in recumbency. Covering the eye with a towel can be a useful adjunct to physical or chemical restraint. If palpable pulse is present, 500 mg prednisolone sodium succinate is administered IV. Assessments of heart rate, pulse quality, mucus membrane color, and capillary refill time are performed. A rapid neurologic examination includes evaluation of panniculus response, anal tone, tail tone, and withdrawal to painful stimuli. If neurologic deficits are not observed, assess "up" limbs for fractures. If no injuries are identified, roll the horse and repeat the limb assessment.
A horse having a "down" leg injury may be sedated, rolled over, restrained, have a splint applied, and be assisted to a standing position.
"Heat Stroke" Post-Exertional Distress Horse
These horses are particularly dangerous because their behavior is highly unpredictable and may range from stuporous to agitated in a very short period of time (Fig. 7). There is a significant safety risk for individuals attending these horses. When possible, minimize the number of people in close proximity to the horse. Facilitated cooling may be achieved through the application and removal of cold water or the use of a cooling blanket [i] The moistened blanket enhances evaporative cooling but is less effective under environmental conditions of high humidity. If water and ice are unavailable, the horse may be doused with rubbing alcohol to enhance evaporative cooling. Although the physiologic mechanism of the distress is not known, affected horses respond clinically to the administration of prednisolone sodium succinate (500 mg) IV. Multiple doses have been administered by the author with no adverse consequences. For violently struggling horses, acepromazine [j] (0.02 mg/kg, IV) or detomidine (30 - 40 μg/kg) may be indicated.

Figure 7. A case of post-exertional distress. (Note that in figure C the bridle has come off and that there seems to be no one responsible for restraining the horse).
7. Euthanasia
On-track euthanasia should be performed only if the veterinarian is absolutely certain that euthanasia is indicated. If there is any question as to whether euthanasia is the correct treatment option, euthanasia is not warranted at that time.
When euthanasia is to be performed on-track or within the confines of the equine ambulance, the author administers 200 mg of succinylcholine [k] IV immediately followed by a 60-ml bolus of euthanasia solution [l]. The use of a large-bore (14 gauge) needle facilitates rapid delivery of the solution. An additional 40 ml of euthanasia solution is administered after the horse is down. Death is confirmed by the absence of corneal reflex, loss of palpable pulse, and cardiac auscultation. If these criteria are not met 60 - 90 s after administration, an additional 50 ml of euthanasia solution is administered.
For racing jurisdictions that do not have a mandated necropsy program, it is advisable to document the nature and extent of the injuries of all euthanized horses. The necropsy area should be removed from any public access areas, enclosed or screened, protected from inclement weather conditions, and have access to running water. Should the euthanized horse be insured or have unknown insurance status, it is advisable to contact the regular attending veterinarian to examine, confirm, and document the injury. When possible, it is advisable not to authorize body removal of an insured horse until contacting the insurance carrier.
8. Conclusion
Management of racing emergencies can be challenging because decisions must be made and plans implemented quickly. Racing emergencies differ little from equine emergencies that occur in other disciplines or under other circumstances. It is the context within which these emergencies occur that provides additional challenges. The well-prepared veterinarian may be surprised when emergencies occur but should not be surprised that they occur. If the veterinarian is not calm, professional, and in control, do not expect that anyone else will be.
Footnotes
- Scollay MC, unpublished data.
- Kimzey Equine Ambulance, Kimzey Welding Works, Woodland, CA 95695.
- Kimzey Leg Saver Splint, Kimzey Welding Works, Woodland, CA 95695.
- dCool Cast, Hawthorne Products, Dunkirk, IN 47336.
- Rompun, Bayer Animal Health, Shawnee Mission, KS 66201.
- Dormosedan, Pfizer Animal Health, New York, NY 10017.
- Telazol, Fort Dodge Animal Health, Overland Park, KS, 66210.
- Solu Delta Cortef, Pfizer Animal Health, New York, NY 10017.
- Cool Medics, Oceanside, CA 92054.
- Promace, Fort Dodge Animal Health, Overland Park, KS, 66210.
- Quelicin, Hospira, Lake Forest, IL 60045.
- Beuthanasia-D, Schering Plough Animal Health Care, Union, NJ 07083.


Comments (0)
Ask the author
0 comments