
How to Perform a Transrectal Ultrasound Examination of the Lumbosacral and Sacroiliac Joints
Updated:
DEC 11, 2013
Languages:
Read
1. Introduction
There is increasing interest in pathology of the lumbosacral and sacroiliac joints giving rise to stiffness and/or lameness and decreased performance in equine sports medicine.1–3 Pain arising from these regions can be problematic alone or in conjunction with lameness arising from other sites (thoracolumbar spine, hind limbs, or forelimbs).4 Localization of pain to this region is critically important through clinical assessment, diagnostic anesthesia, and imaging.
In general, diagnostic imaging of the axial skeleton and pelvis is difficult to perform and to interpret. Radiography is infrequently performed. To obtain good-quality diagnostic radiographs, general anesthesia, a high-output radiographic generator, and special techniques must be performed.5,6 Variation in the size and shape of the sacroiliac joints and sacral wings and caudal sacral osteophytes are common7,8; special techniques for taking radiographs have allowed for identification of these structures and the inter-transverse joints.5 These authors urge caution in the interpretation of lesions identified on radiography in the absence of other diagnostic imaging and clinical examination. Nuclear scintigraphy is an important component of work-up for sacroiliac region pain, but limitations exist. Several reports9,10 exist detailing the anatomy and technique findings in normal horses11,12 and findings in lame horses.13 Patient motion, camera positioning, and muscle asymmetry can cause errors in interpretation. In normal horses, the appearance of the sacroiliac region varies with age but is generally symmetric. In horses with sacroiliac problems, it is more difficult to distinguish the tubera sacrale from the sacroiliac joint than in normal horses, and, in horses with lameness, there is more asymmetry detected.12,13
Techniques for percutaneous and transrectal ultrasound examination have been described, and their use is increasingly common.2,14-19 Ultrasound is very useful for the evaluation of the joint margins and lumbosacral intervertebral disc.14 Similar to the radiographic anatomy of the region, variability exists in the appearance of the tubera sacrale, dorsal sacroiliac ligaments, thoracolumbar fasciae, and the lumbosacral joint.3,19 Artifacts of acquisition and interpretation can occur with improper technique in the ultrasound examination, and knowledge of reference images and the regional anatomy is paramount in accurate interpretation of diagnostic imaging studies of this region. All diagnostic imaging techniques should also be interpreted in light of the anamnesis and the static and dynamic clinical examination.
The purpose of this “How-to” presentation is to provide a review of the technique for transrectal ultrasound with reference images and ultrasound images of examples of pathology of the lumbosacral junction, lumbosacral intertransverse joints, and sacroiliac joints. This presentation will review imaging findings in 231 horses presenting to Lingehoeve Diergeneeskunde, Equine Referral Hospital, The Netherlands, for evaluation of stiffness or poor performance in 2012.
2. Materials and Methods
The diagnostic imaging picture archiving and communications system (PACS) of Lingehoeve Diergeneeskunde was searched for all horses undergoing transrectal ultrasound during 2012. Age and breed data were collected. All horses had a complete clinical evaluation for poor performance. After anamnesis and static and dynamic examination, a percutaneous examination of the lumbar spine and a transrectal examination of the sacroiliac and lumbosacral junction were performed.
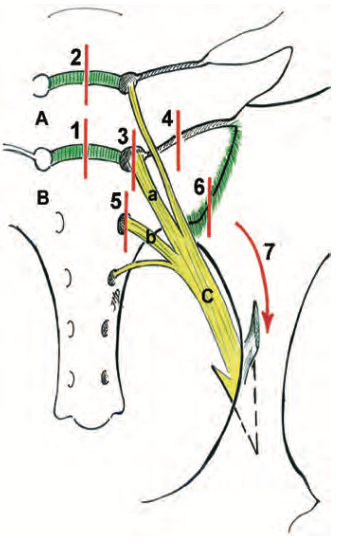
Transrectal ultrasound examination was performed with the use of the technique described by Denoix.20 and illustrated in Fig. 1. A 5- to 10-MHz micro-convex intra-operative ultrasound probe was used per rectum. All horses were sedated with an α-2 agonist and restrained in stocks. The rectum was cleaned, and copious lubricant was introduced into the rectum. A stand-off pad was not used. Anti-spasmodic agents were used infrequently (nine horses). The ultrasound images are oriented so that ventral is to the bottom of the image display screen, and, when appropriate, cranial is to the left.
Fig. 1. Schematic drawing by Denoix of the ventral aspect of the lumbosacral region illustrates the stepwise procedure of transrectal evaluation of the lumbosacral and sacroiliac joints. Red lines indicate probe orientation. A, Sixth lumbar vertebra; B, sacrum; C, sciatic nerve; a, L6 nerve root; b, S1 nerve root; 1, lumbosacral intervertebral joint; 2, L5–6 intervertebral joint; 3, lumbosacral intervertebral foramen; 4, lumbosacral intertransverse joint; 5, S1–2 intervertebral foramen; 6, sacroiliac joint; 7, direction of imaging the psoas minor tendon.
Technique
Step 1: Lumbosacral Disc
Transrectally, the aorta and its bifurcation (normally at the level of the fifth lumbar vertebra) can be palpated. Place the ultrasound probe in a median plane, caudal to the aorta and vena cava (bifurcation normally at the level of L5). The L6 and S1 vertebrae can be recognized by the well-defined hyperechoic shadowing ventral margins, meeting at approximately a 140° to 150° angle. At this site,
the lumbosacral (LS) disc, the ventral longitudinal ligament, and, occasionally, the dorsal longitudinal ligament, can be identified (Fig. 2). At this location, scan the entire disc by moving the probe left and right, maintaining a paramedian orientation of the probe.
Step 2: Intervertebral Disc and Vertebral Bodies of L5–6 and L4–5
From the LS disc, move the ultrasound probe in a cranial direction while maintaining the median plane orientation. As the probe is moved forward, maintain visualization of the ventral vertebral margin. The L5– 6 disc is just dorsal and is usually caudal to the aortic bifurcation. The probe is moved cranially to identify the L4 –5 disc space dorsal to the aorta.
Step 3: Lumbosacral Intervertebral Foramen
Identify the LS disc space. Move the probe in a lateral direction, maintaining a paramedian imaging plane. As the probe is moved laterally, look for a smoothly demarcated defect in the bone surface that represents the intervertebral foramen. [...]
About
How to reference this publication (Harvard system)?
(2013) “How to Perform a Transrectal Ultrasound Examination of the Lumbosacral and Sacroiliac Joints”, AAEP Annual Convention - Nashville, 2013. Available at: https://www.ivis.org/library/aaep/aaep-annual-convention-nashville-2013/how-to-perform-a-transrectal-ultrasound-examination-of-lumbosacral-and-sacroiliac-joints (Accessed: 24 April 2024).
Author(s)



Copyright Statement
© All text and images in this publication are copyright protected and cannot be reproduced or copied in any way.Provided by:

Comments (0)
Ask the author
0 comments